You want clear answers: which device works for your condition, how they differ, and what evidence backs each claim. At surface level both aim to change nervous-system activity, but they do it with different hardware, signals, and clinical histories. Picture two musicians: one plucks the vagus nerve directly with implanted strings (precise, invasive), the other plays steady rhythms at the body’s periphery to coax a sympathetic-parasympathetic duet (noninvasive, variable). That analogy hides a surprising truth: some noninvasive rhythmic tools can produce clinically meaningful shifts in heart rate variability and mood, while implanted vagus nerve stimulators (VNS) have decades of regulated outcomes. Read on to understand mechanisms, what the research says, safety trade-offs, and how you might choose between them.
How Each Device Works: Mechanisms And Technology
Fact: Vagus nerve stimulators deliver targeted electrical pulses to change efferent and afferent signaling: rhythmic resonance devices use patterned sensory input to entrain autonomic rhythms.
Vagus Nerve Stimulators: Mechanism, Components, And Delivery
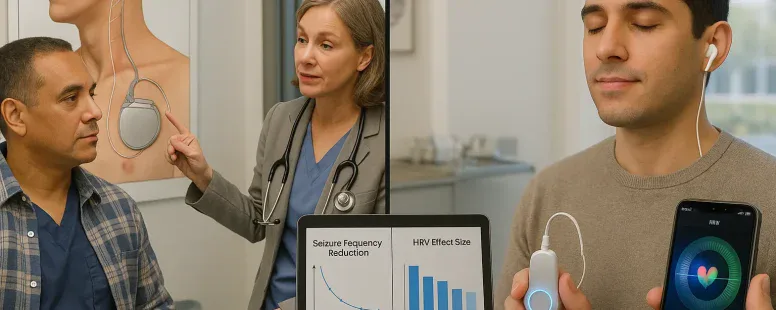
VNS devices (brands: LivaNova, NeuroPace historically, some investigational systems from Medtronic) use an implanted pulse generator and a cuff lead wrapped around the cervical vagus. The device sends short electrical pulses (typically 20–30 Hz for conventional VNS, but parameters vary) to activate A- and B-fibers. You get direct modulation of brainstem nuclei (nucleus tractus solitarius, locus coeruleus) and downstream changes in neurotransmitters like norepinephrine and GABA. The delivery is invasive: surgical implantation under general anesthesia, a subcutaneous pulse generator, and leads tunneled to the neck. Programming adjusts amplitude, frequency, pulse width, and duty cycle to balance efficacy and side effects.
Rhythmic Resonance Devices: Theory, Waveforms, And Modalities
Rhythmic resonance devices include transcutaneous auricular vagus nerve stimulation (taVNS), wearable breath pacers, HeartMath biofeedback systems, binaural-beat headsets, and cranial electrical stimulators (e.g., Fisher Wallace). They present patterned stimuli, mechanical, electrical, auditory, to peripheral receptors with the goal of entraining cardiorespiratory or neural rhythms. For example, taVNS delivers pulses to the cymba conchae (auricular branch of the vagus) at lower intensities and varied frequencies (often 1–25 Hz). HeartMath trains paced breathing around ~0.1 Hz (6 breaths per minute) to boost heart rate variability (HRV). The devices are mostly noninvasive and you can use them at home.
Key Physiological Differences And Overlapping Pathways
Direct VNS recruits deep cervical fibers and produces robust afferent signaling into central autonomic networks. Rhythmic devices often recruit peripheral mechanoreceptors, cutaneous vagal branches, and baroreflex pathways indirectly. Both can increase parasympathetic markers (higher HRV) and reduce sympathetic reactivity, but the magnitude, latency, and consistency differ. VNS gives stronger, more reproducible central effects: rhythmic resonance tools rely on entrainment and behavioral coupling, so results vary with compliance and context.
Clinical Uses And Indications
Fact: VNS holds formal regulatory approvals for epilepsy and treatment-resistant depression: rhythmic resonance approaches have fewer formal approvals but many off-label and wellness applications.
Regulatoryly Approved Indications For Vagus Nerve Stimulators
The U.S. Food and Drug Administration (FDA) has cleared implantable cervical VNS for focal epilepsy (since the 1990s) and for treatment-resistant major depressive disorder (2005, with more recent labeling updates). LivaNova’s VNS system is a leading example. Approvals mean you can expect standardized surgical pathways, reimbursement codes (CPT/DRG contexts), and long-term registries tracking outcomes.
Emerging And Off-Label Uses For Both Modalities
Clinicians use VNS off-label for cluster headache, Alzheimer’s disease trials, obesity, and PTSD. Rhythmic resonance devices see use for anxiety, insomnia, chronic pain, and stress reduction, often in primary care or behavioral health settings. You will find growing clinical trials testing taVNS for inflammatory conditions and migraine.
Conditions Where Rhythmic Resonance Devices Show Promise
Devices that alter breathing or peripheral vagal input show signal in anxiety disorders, PTSD symptom clusters, and cardiovascular risk reduction (via improved HRV). HeartMath has corporate wellness data: randomized trials of paced breathing show short-term anxiety and blood pressure benefits. taVNS has pilot RCTs suggesting mood and pain benefits, but you should note sample sizes are often small and results mixed.
Evidence, Outcomes, And Comparative Effectiveness
Fact: High-quality randomized trials exist for implantable VNS: data for rhythmic resonance devices are promising but more heterogeneous.
Summary Of Major Clinical Trials For VNS
Large, long-term studies in epilepsy demonstrate reduced seizure frequency by ~50% in many responders after months to years. For treatment-resistant depression, VNS produced modest but durable response rates in open-label and registry data versus treatment as usual: randomized controlled trial evidence is more nuanced. Key trials include multicenter cohorts tracked in national registries and device manufacturer-sponsored outcomes studies.
Summary Of Major Studies For Rhythmic Resonance Devices
You’ll find many small RCTs and crossover studies for paced breathing, HRV biofeedback, and taVNS. Meta-analyses of HRV biofeedback report moderate effects on anxiety and depression symptoms: taVNS meta-analyses show small to moderate effects but high heterogeneity. Auditory approaches (binaural beats) show inconsistent results: some studies report mood shifts, others find no effect. The common limitation is small samples and variable sham controls.
Direct Comparative Data And Gaps In Research
Head-to-head trials comparing implantable VNS and rhythmic resonance devices are essentially absent. You can infer that implanted VNS produces stronger central modulation, but you can’t directly compare patient-centered outcomes across consistent protocols. Major gaps: standardized dosing for taVNS, long-term randomized studies of rhythmic devices, and pragmatic trials that test scalability and adherence. Future studies should include biologic markers (HRV, inflammatory cytokines) and patient-reported function.
Safety, Side Effects, And Contraindications
Fact: Implantable VNS carries surgical and device risks: noninvasive rhythmic devices have milder, mostly transient side effects.
Device-Specific Risks And Common Adverse Effects
Implantable VNS: surgical risks (infection, lead migration), voice changes/hoarseness (common), cough, dysphagia, and hardware malfunction. Rarely, cardiac effects occur if programming is aggressive. Brands with strong postmarket surveillance (LivaNova) provide detailed adverse event tables. Noninvasive rhythmic devices: skin irritation with taVNS, headache, dizziness, transient insomnia, and rare mood shifts. Home-use cranial stimulators sometimes cause nausea.
Contraindications, Monitoring, And Management Strategies
You should avoid implantable VNS in patients with high surgical risk or active infection. Monitor voice changes and wound healing post-op: device interrogation is needed periodically. For taVNS and electrical cranial stimulators avoid use in people with implanted cardiac pacemakers or unstable cardiac arrhythmias unless cardiology clears it. Always screen for a history of syncope. If adverse effects occur, reduce amplitude, change duty cycle, or pause therapy.
Long-Term Safety And Device Maintenance Considerations
Implanted generators need battery replacement every 5–10 years depending on settings. Leads can fail and require revision. Noninvasive devices need periodic calibration and safe-charging habits: software updates and app privacy policies matter. You’ll want structured follow-up: device checks for implants, adherence coaching for wearables.
Practical Considerations For Patients And Clinicians
Fact: Choice between implantable and noninvasive options depends on severity, prior treatment response, and your tolerance for invasive procedures.
Implantable Versus Noninvasive Options: Procedure, Recovery, And Lifestyle Impact
Implantation involves surgery, a short recovery, and possible activity restrictions for weeks. You may need MRI conditional planning: some VNS systems are MRI-conditional with manufacturer guidelines. Noninvasive devices let you start at home, require training, and need daily time commitments. Lifestyle impact is higher with an implant up-front: long-term you might forget you have a generator. Costs and recovery differ sharply.
Patient Selection, Shared Decision-Making, And Informed Consent
You should weigh prior medication and therapy failures, comorbidities, and goals. Shared decision-making must include realistic expectations, alternative options (e.g., rTMS, CBT), and potential lifestyle trade-offs. Use decision aids, involve family, and document consent specifics about battery replacements and revision risks.
Cost, Access, Reimbursement, And Follow-Up Care
Implants have higher upfront costs but are often covered for FDA-approved indications: check payer policies. Noninvasive devices vary: some covered as durable medical equipment, many sold direct-to-consumer (out-of-pocket). Follow-up differs: implanted device clinics versus remote app-based monitoring. Plan for long-term care pathways and data privacy concerns.
Future Directions And Innovations
Fact: The field is moving toward personalization, closed-loop control, and hybrid approaches that blend implants with wearable sensing.
Technological Advances, Personalization, And Closed-Loop Systems
Next-gen systems aim to record physiologic signals (EEG, HRV) and deliver stimulation only when needed. Closed-loop VNS prototypes trigger pulses based on seizure onset or arrhythmia precursors. Personalization will tune waveforms to your biometrics, improving efficacy and reducing side effects.
Research Priorities, Regulatory Trends, And Clinical Adoption
You should watch for larger RCTs of taVNS with standardized protocols, and registries that compare devices in real-world settings. Regulators (FDA, EMA) are increasingly asking for patient-centered outcomes and long-term safety data before broad approvals. Clinical adoption will depend on reimbursement and robust comparative-effectiveness evidence.
Practical Outlook: How To Watch For New Evidence And Decide When To Adopt
Track clinicaltrials.gov for active trials, read FDA summaries for device clearances, and follow professional society guidelines (AAN, APA). If you’re considering therapy, consult a multidisciplinary team, neurology, psychiatry, cardiology, review the latest trials, and try noninvasive options first if you prefer lower immediate risk. Be honest about what you can commit to: adherence matters more than device sophistication. Sometimes the simplest paced-breathing practice gives measurable benefit, don’t dismiss it while waiting for the next device to arrive.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behaviour or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.